IVF & Fertility Treatments
After a thorough work up, we will help determine which treatment is right for you.
Not only does this personalised approach save you costs, it saves you time and increases your chances of a successful outcome.
Assisted Reproductive Technology (ART) services available at Coastal IVF:
Ovulation Induction and Intra-Uterine Insemination (OI / IUI)
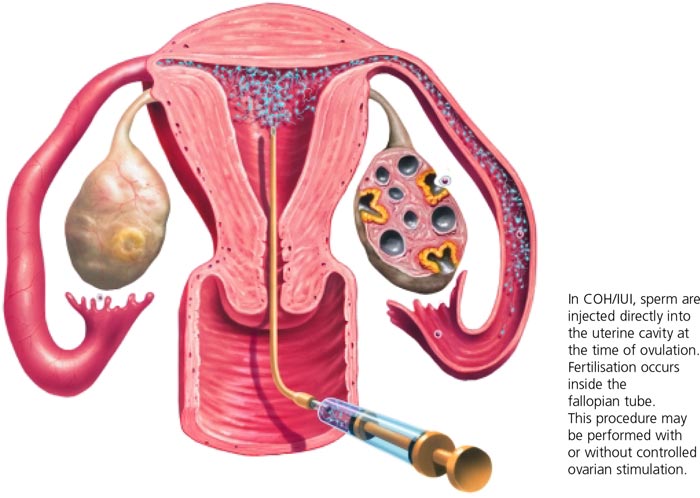
Stimulation of the ovaries (ovulation induction) to release an egg followed by the introduction of prepared sperm into the uterus via intra-uterine insemination. This is used for patients with an ovulatory defect.
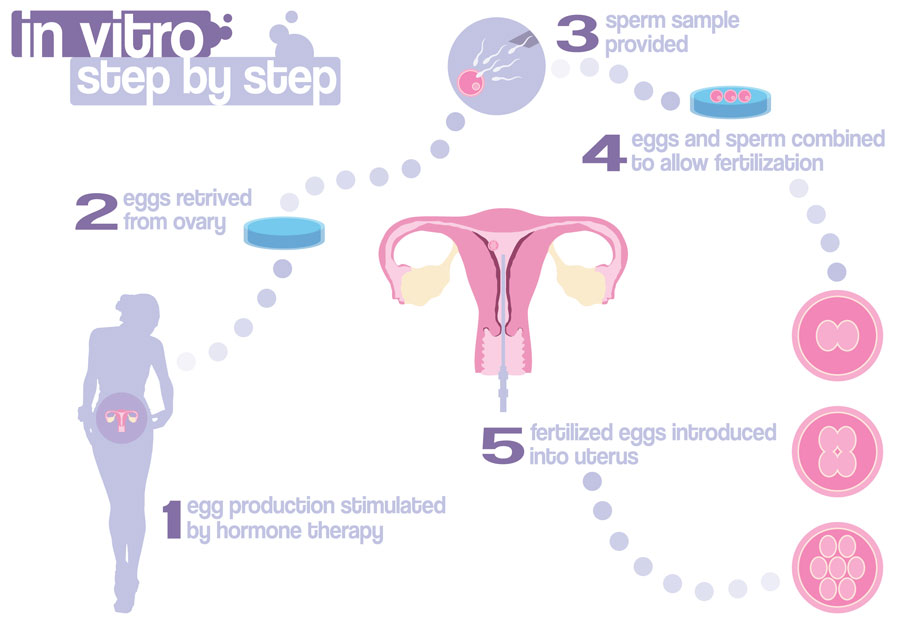
In Vitro Fertilisation (IVF)
IVF involves stimulation of the ovaries (via medications) to develop 10-15 mature follicles. Immediately prior to ovulation, these follicles are aspirated under anaesthesia to retrieve the eggs (known as oocytes). These oocytes are combined with sperm in the laboratory to allow fertilisation. After 3-5 days of growth, an early embryo is then transferred into the woman’s uterus and hopefully implantation occurs.
Intra-Cytoplasmic Sperm Injection (ICSI)
In certain situations, the sperm are unable to fertilise an egg. In these cases, ICSI can be used (as an addition to IVF) to aid fertilisation by retrieving and injecting a single sperm directly into an egg.
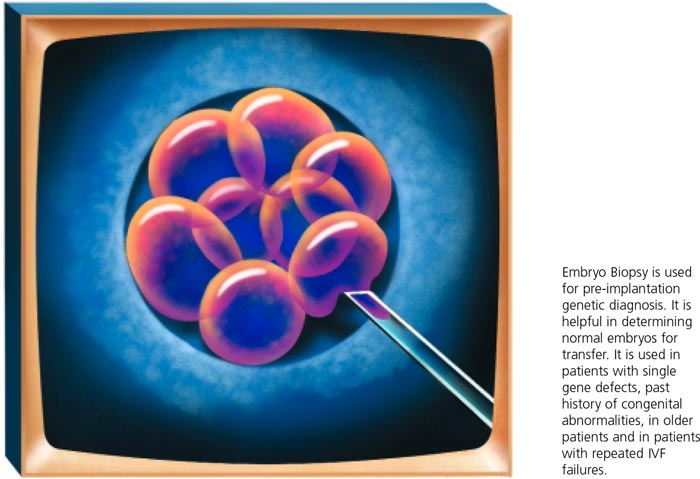
Pre Implantation Genetic Testing (PGT)
Pre-implantation genetic testing (PGT) may be used to identify genetic abnormalities in the embryo like aneuploidy (abnormal number of chromosomes) or inheritable conditions such as cystic fibrosis. This enables clinicians to transfer unaffected embryos and improve the chances of a successful pregnancy.
Sperm, oocyte and embryo freezing (cryopreservation)
Sperm, oocytes and surplus embryos may be frozen and stored for use in future treatment cycles, or donated to couples that need these to conceive.
We know all of this may seem overwhelming, but we are here to help you understand your options and make the process simple.
If you would like more detailed information on each option, simply take a look through the tabs below.
Treatments in Detail:
Ovulation Induction and Intra-Uterine Insemination
Ovulation induction (OI) is often used for women an ovulation defect, which is one of the most common causes of sub- or infertility. Ovulation issues are especially prevalent in women with polycystic ovaries, endometriosis and older age.
OI uses oral medications to increase the brains natural production of FSH (follicle stimulating hormone). FSH recruits and grows ovarian follicles, and this is monitored by regular ultrasounds. Once a dominant follicle is large enough, ovulation may occur spontaneously or will be induced with an injection.
Intrauterine insemination (IUI) is then performed a day later (around the time of ovulation). This is done by preparing sperm (to concentrate the healthy spermatozoa) and placing them in the uterus via a soft catheter.
Pros and Cons of OI/ IUI:
- Less invasive and less medications than IVF
- Much lower cost than IVF
- Minimal laboratory involvement (closely simulates normal physiology)
- Lower success rates (per cycle) compared to IVF
- Less diagnostic information than IVF (not able to assess fertilisation or embryo development)
In Vitro Fertilisation
IVF is often promoted as the only option for patients seeking fertility treatment or assistance becoming pregnant. Whilst effective and popular, IVF is more invasive, has greater risks and costs compared to alternatives such as OI/ IUI. At Coastal IVF we don’t push patients into IVF and we believe it should be reserved for those that need it.
Coastal IVF has one of the highest success rates with IVF in the country, and we are so confident in our processes that we offer a second cycle guarantee – this means no out of pocket costs on a subsequent cycle (if you need it)!
IVF – The Process
- Down regulation
- Various medications and regimes may be used to ‘quiet’ your ovaries and stop the normal cyclical recruitment and growth of ovarian follicles. This is an essential step so that when we start stimulation, we can recruit as many follicles at similar sizes.
- Ovarian stimulation
- Injections of FSH (follicle stimulating hormone) are used to recruit and grow ovarian follicles. The goal is to have around 10-15 dominant follicles at the time of oocyte (egg) retrieval.
- Oocyte retrieval (egg pickup)
- Under anaesthesia, a long needle is used to retrieve eggs from each follicle.
- In vitro fertilisation and embryo culture
- Retrieved oocytes are fertilised with sperm in the laboratory and then incubated and monitored until around day 5 of life. At this stage they are known as a ‘blastocyst’
- Embryo transfer
- Embryos are transferred usually 3-5 days after egg retrieval into the women’s uterus and hopefully an implantation occurs.
- Luteal support and monitoring for pregnancy
- Medications are often given to support the early pregnancy and a blood test (b-hCG) is performed around 12-14 days after transfer to check for pregnancy.
Key requirements, pros and cons of IVF
- More demanding than OI / IUI
- Suitable for almost all forms of infertility
- Better success rates per cycle than OI / IUI
- More diagnostically informative than OI / IUI
- May need sperm injection (ICSI) to assist fertilisation
Did you know? Reproductive techniques were revolutionised by the birth of Louise Brown in 1978. This was the world’s first IVF birth and Louise was delivered by a mother who did not have fallopian tubes. This is the routine treatment now offered to patients whose tubes are not suitable for tubal surgery or if tubal surgery has failed.
Intracytoplasmic Sperm Injection
ICSI is a technique in which a single sperm is captured using a fine needle and injected into an egg to cause fertilisation. This is used in cases of male factor infertility where usual fertilisation is impaired.
It is important to recognise that ICSI is an addition to conventional IVF, not an alternative.
Key benefits
- Used to assist fertilisation in cases where it cannot be achieved using conventional in-vitro fertilisation techniques (e.g low sperm count, poor sperm motility or where a vasectomy has previously been performed)
- With ICSI, fertilisation and pregnancy rates in these cases may be comparable to conventional IVF with normal sperm parameters.
- This service is now covered by a Medicare rebate

Testicular Sperm Aspiration
This is a procedure for azoospermic (no sperm in the ejaculate) men. Under local anaesthetic, sperm are extracted directly from the testicle using a fine needle biopsy technique. ICSI is then used to achieve fertilisation.
This procedure can enable some couples (who would otherwise need donor sperm), to achieve a pregnancy with their own genetic material. This is useful in men with prior vasectomy or certain conditions that affect spermatogenesis.
The male requires initial investigations to see if this is an appropriate procedure for him, this involves a physical examination and hormonal profile (a blood test). There may also be a role for chromosome analysis and/or genetic counselling.
TESA is the biopsy technique of choice in men with obstructive azoospermia and replaces the more invasive open biopsy technique. It has a very low complication rate and a rapid recovery.
Frozen Embryo Transfer (FET) Cycle
After a stimulated IVF cycle, there may be a surplus of embryos that can be cryopreserved and used for future cycles. Frozen embryo transfer (FET) cycles begin by preparing the lining of the uterus (the endometrium) to receive a pregnancy. This is done by the natural cycle, ovulation induction or hormonal replacement therapy (HRT).
Once the endometrium is ready, the embryos are thawed and then transferred into the uterus and hopefully implantation occurs. With the advancement of freezing and thawing technologies, FET cycles now have similar success rates to fresh transfers.
Pre-implantation Genetic Testing
- Pre-implantation Genetic Testing (PGT) involves the removal of one or two cells from an embryo to examine the cells for specific chromosomal abnormalities.
- The embryos are biopsied in our laboratory but the cells are sent away to genetic laboratories for analysis. This takes time so PGT requires all embryos to be frozen until the results are received and then a FET cycle can be performed.
- PGT allows us to identify the unaffected embryos for transfer in order to increase successful pregnancy rates (per transfer).
What is Assisted Reproduction Technology (ART)?
ART treatment comprises of 3 cycle phases:
1) Ovulation/Ovarian Stimulation
The ovulation induction or ovarian stimulation phase where the growth of immature eggs in the ovary is tracked using hormone monitoring and ultrasound imaging. This phase includes the use of drugs to take control of ovarian physiology and stimulate the development of several eggs in a controlled manner. However, mild or no ovarian stimulation can also be used if so desired. The growth or stimulation phase occurs in the first part of the menstrual cycle, although some drugs may be administered in the late part of the previous menstrual cycle in order to take control of ovarian physiology. The whole phase lasts between 2 – 4 weeks depending upon the form of treatment employed. The Assisted Reproduction Technology phase begins around mid cycle and can take up to 6-7 days in the case of blastocyct culture or 3-4 days for cleavage stage embryo transfer. This is where one of the following procedures will be employed.
2.1) Intra-Uterine Insemination (IUI)
2.2) In Vitro Fertilisation (IVF) and Embryo Transfer (ET)
2.3) Frozen Embryo Transfer (FET)
These ART procedures are summarized below with more detailed descriptions of each technique.
Also see OPU and ET for information about the egg pick and embryo transfer.
3) Luteal Phase
The luteal phase corresponds to the second half of the menstrual cycle and involves the administration of injections or vaginal pessaries to assist the development of a suitable endometrium in the uterus for the embryo to implant into. Contrary to popular belief implantation of the embryo does not occur at the time of replacing the embryos into the uterus, but occurs a few days later. Pregnancy testing is performed at the end of this phase (16 days after egg pick-up).

Luteal Phase Support (2 week support)
Surviving The Wait
The two weeks following embryo transfer can often be an arduous time awaiting your pregnancy test. During this phase we may give medication by injection or pessaries or a vaginal gel to maintain the lining of the uterus to assist implantation and possibly improve the chances of pregnancy.
During this stage you may visit the nurse coordinator who will check your well being and give moral support. At any of these stages please feel free to contact our clinic if you have any concerns. You may resume normal activities the next day following the transfer. Regular exercise and minimal stress is recommended.
All couples enter these treatment programs with high hopes and dreams of a family. It would be wonderful if everyone could conceive simply and without fuss. The reality is that pregnancy rates in all reproductive treatments are only around 30%, so treatments can be prolonged and fraught with disappointment, frustration, depression and anger. Success rates are also significantly dependant upon the age of the female partner, with pregnancy rates declining significantly in women aged in their late thirties or older. It is important to bear in mind that in a highly fertile couple the best pregnancy rate that can be achieved in a single cycle, under ideal conditions with correctly timed intercourse, is around 20%. We will give you an honest assessment of our views of what your chances may be and indeed one treatment cycle often enlightens us as to the specifics of your infertility and what modifications may improve your prospects in future cycles.